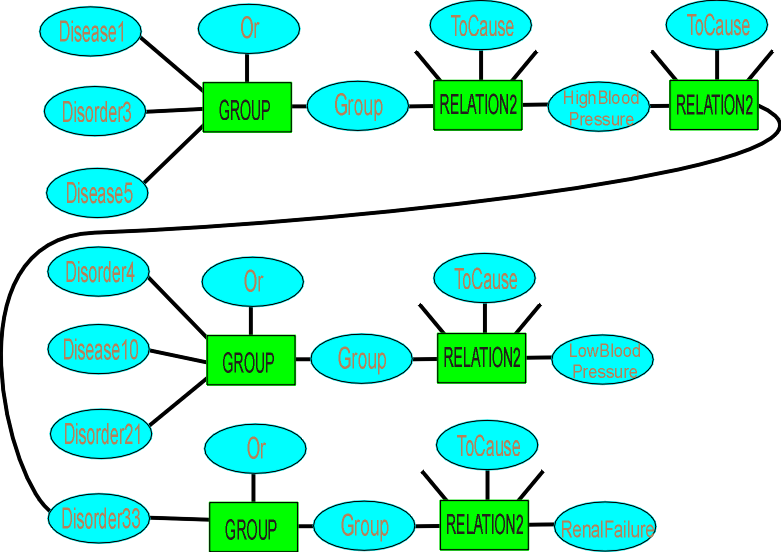
We have diseases and disorders causing symptoms (and some of the symptoms themselves causing disorders), which gives
This is a temptingly simple structure, but some disorders cause a rapid change in symptom and then plateau, some take years with slow rise and no plateau (except death). The rate of onset is a useful marker (it means looking at old notes is useful). Only where diseases and disorders show exactly the same symptom path should we group them (for that symptom). And "High Blood Pressure" is itself too crude – is it high diastolic pressure coupled with high systolic pressure, or is the systolic pressure low? And is the pulse rate elevated, is the patient in a resting state (and not recovering from strenuous exertion)? We are looking for patterns, rather than one symptom switching.
The diagram is instructive in one way – there will be multiple diseases for every symptom and we need to go back to the possible disease and then forward to its other symptoms to differentiate among the potential diseases and disorders. Where we have consequential disorders, many of them will have thresholds, so the other disease/disorder will have to have existed for some time. We may need to hypothesise about a disease, and to hypothesise for a certain time period, not just switch it on – if they have had this disease for three months (they didn’t have any symptoms at the last checkup six months ago), then we should see ….
This makes the representation of each disease a much more complex thing – times and symptoms will depend on the patient – a child, a frail old person (bones easily broken, reduced immune system activity), a bedridden person. A lot of this can be done with states, but many states interact to make the situation worse – old, frail, bedridden and pneumonia. We not only have to provide a diagnosis, we have to provide a prognosis – are they going to die in a day, a week, or should all efforts be directed at curing some other disease they have which has a higher priority?
There may be more than one disease or disorder – a pure case will be unusual.
Timelines are important –the patient may be worn down by the disease.
States may not be independent – age, health, blood pressure.
Functions may not be monotonic – susceptible in childhood and old age (perhaps due to different factors – a not yet fully functioning immune system, or one grown tired).
A disease or disorder may have led to another, which may be more life-threatening than the original, and if cured, will recur unless the original disease/disorder is cured.
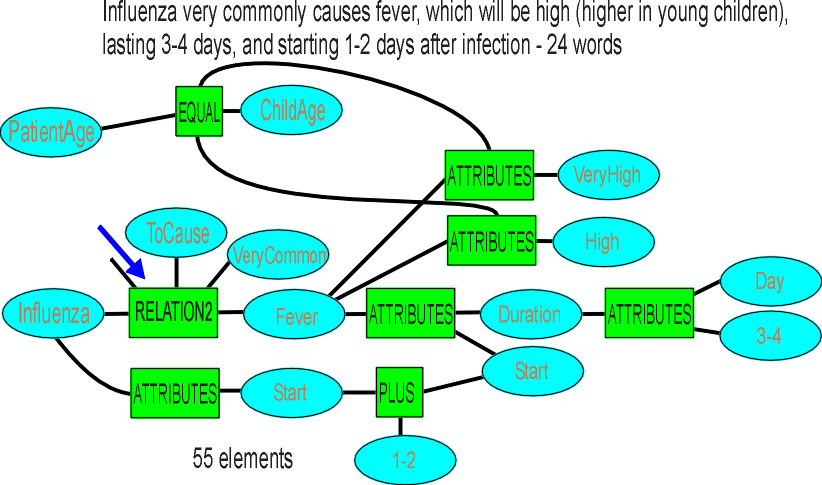
Take influenza as an example.
Already there are different strains – bird flu, swine flu, normal flu. There is some immunity in the population for a slowly evolving strain.
Here is a comparison for symptoms of flu, the common cold, allergy.
URI, seasonal allergies, influenza: symptom comparison |
|||
Symptoms |
Allergy |
URI |
Influenza |
| Itchy, watery eyes | Common | Rare (conjunctivitis may occur with adenovirus) | Soreness behind eyes, sometimes conjunctivitis |
| Nasal discharge | Common | Common | Common |
| Nasal congestion | Common | Common | Sometimes |
| Sneezing | Very common | Very common | Sometimes |
| Sore throat | Sometimes (postnasal drip) | Very common | Sometimes |
| Cough | Sometimes | Common (mild to moderate, hacking) | Common (dry cough, can be severe) |
| Headache | Uncommon | Rare | Common |
| Fever | Never | Rare in adults, possible in children | Very common (100-102�F (or higher in young children), lasting 3–4 days; may have chills) |
| Malaise | Sometimes | Sometimes | Very common |
| Fatigue, weakness | Sometimes | Sometimes | Very common, can last for weeks, extreme exhaustion early in course |
| Muscle pain | Never | Slight | Very common, often severe |
We are going to need spectra in several dimensions on some symptoms, such as coughing. We can have slight to mild to moderate to severe, dry to productive, hacking or not, a probability of occurrence of rare, sometimes, common, very common (an existence value, but related to whether Influenza is true, not in general). Never will be represented as no connection.
So what does the table look like if we fully represent it? And how will its application to "young children" or "adults" be represented – that is, the function wants to know who’s asking? The patient is a static construct, set up at the beginning of the consult, so that is not too hard.
We have to be careful not to let the number of elements get away from us, while simultaneously doing an adequate job of knowledge representation.
We can group all the Very Common symptoms of Influenza, to get
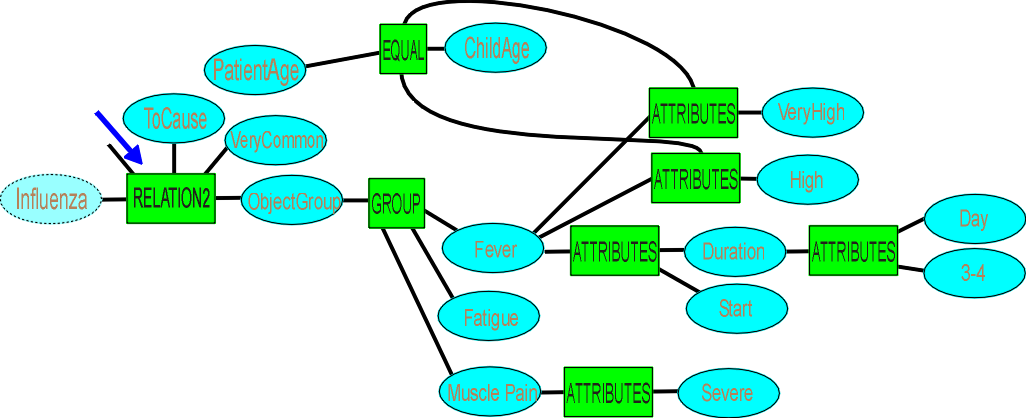
The diagram isn’t handling "often severe" for muscle pain – we could make it range from moderate to severe.
And where we have common causes, common probabilities and a single symptom:
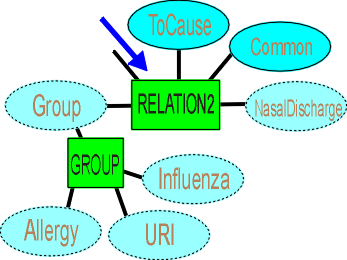
If we hypothesise Influenza, we set it to exist, which causes the Group to exist (it has an Any control), which causes a Nasal Discharge. If we don’t have Nasal Discharge as a symptom, it lessens the probability of Influenza (we have an Uncommon case, or not at all).
This should cut down on the number of elements considerably. It means we will be continually reorganising the structure to be more efficient. It will also force us to ungroup objects where we get better information on one disease, and have to dedicate a relation purely to it.
How much more would we need to know about Influenza? Viral disease, may cause pneumonia, which may be fatal for very young and very old.
Let’s say we use 150 elements on average per disease or disorder (after using any existing structure), and have 2000 diseases/disorders in the TriageGP unit (out of a total of about 6000). That gives us:
Grammar 100,000 (to be able to read text)
Body parts 100,000
Symptoms 100,000
Diseases/disorders 300,000
Treatments 200,000
Total 800,000
This looks possible, as long as we are reasonably frugal with elements.
We probably need some priority and depth for potentially fatal diseases.
The specialty units will have more depth on their special diseases – we have to be able to differentiate, and push pills or recommend simple remedies where that is appropriate.